Healthcare Burns $12.5 Billion on Outdated Claim Status Checks
While staff play portal hopscotch for 24 minutes per claim, AI finds critical cases in 320 milliseconds—guess which approach saves billions?
The $12.5 Billion Question: Why Healthcare Still Checks Claim Status Like It's 1999
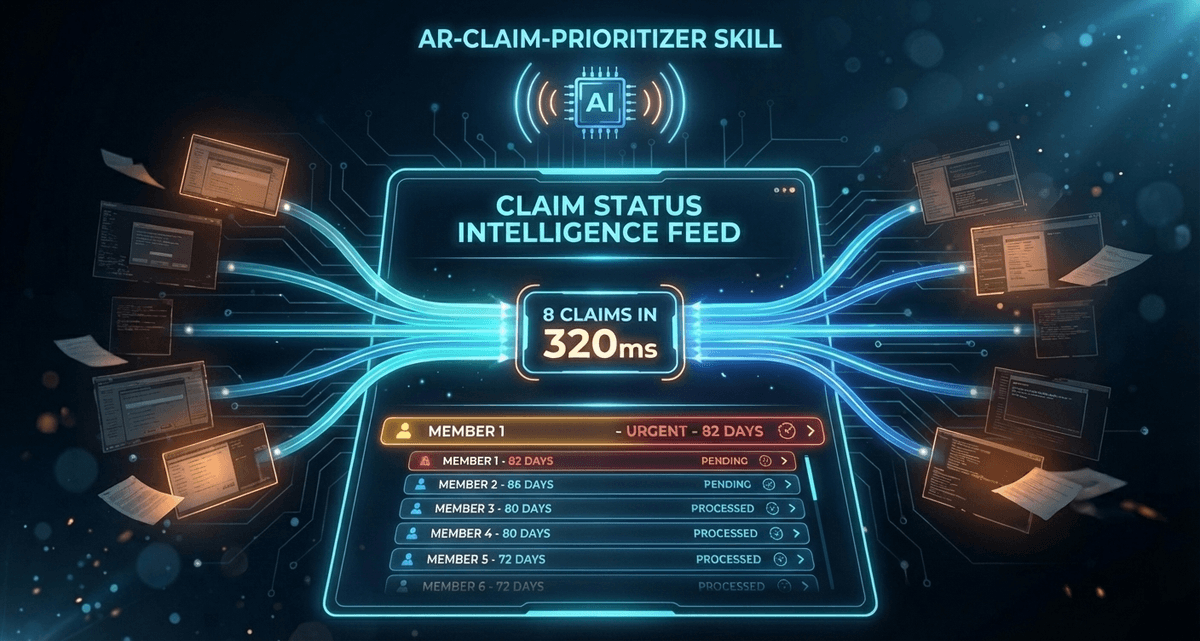
Dorothy Washington's claim sat 82 days outstanding, just 8 days from the timely filing cliff. No human had checked her status in weeks. Then AI found her in 320 milliseconds, flagged the risk, and queued the action. Meanwhile, across town, a billing specialist was still logging into Portal #7 of her morning routine, squinting at cryptic status codes that might as well be hieroglyphics.
This is healthcare's most expensive morning ritual: the great portal refresh marathon that's burning through $12.5 billion annually while Dorothy Washington's claim ticks toward write-off status.
The Hidden Labor Tax Crushing Healthcare Billing
Healthcare just spent $12.5 billion on claim status inquiries in 2023, a 71% jump that represents more than just inflation. It's the cost of a fundamentally broken workflow where 36% of billing staff touches involve nothing more sophisticated than checking whether a payer has processed a claim.
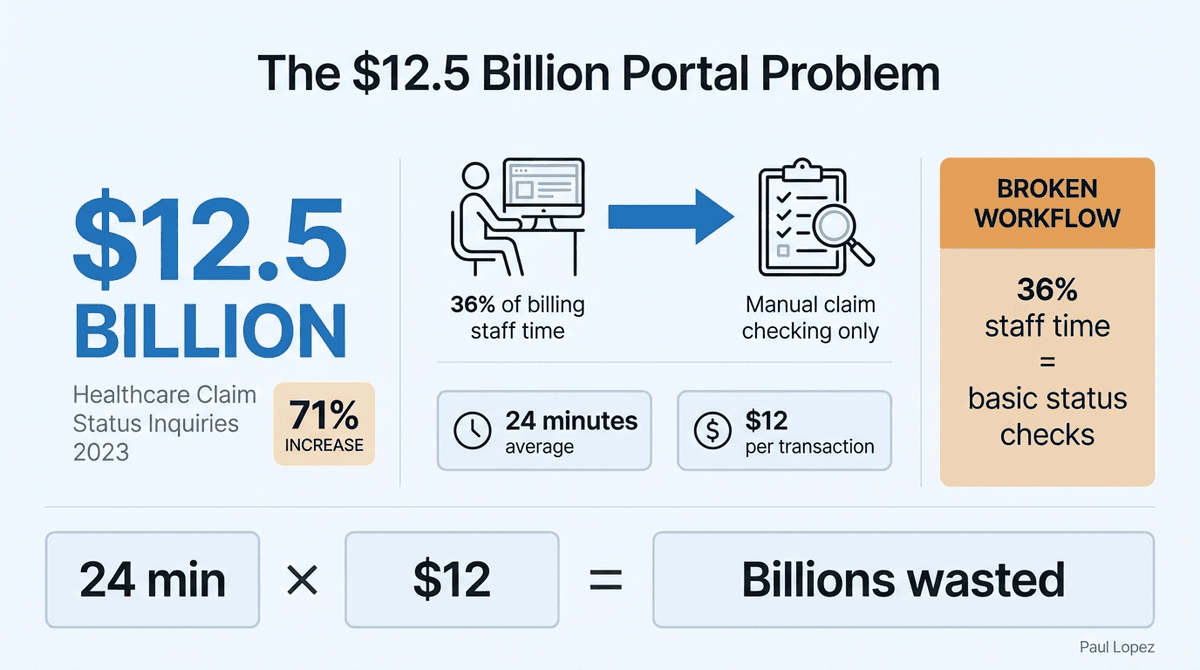
The math is brutal but simple. Each manual claim status inquiry averages 24 minutes at $12 per transaction. Multiply that across millions of claims, factor in the average practice juggling 12 different payer portals, and you get an industry stuck in a Groundhog Day loop of administrative busy work.
Here's what makes this particularly maddening: the standards to automate this process have existed for decades. HIPAA 276/277 claim status transactions were codified specifically to eliminate manual portal checking. But having electronic adoption (currently at 74%) doesn't mean having intelligent automation. Most practices get faster data retrieval, not smarter prioritization.
The Dorothy Washington scenario illustrates the real cost. While billing specialists burn hours checking routine claims that are processing normally, high-risk claims approach critical deadlines unnoticed. Timely filing denials represent 4-7% of all claim denials, yet they're almost entirely preventable with proper monitoring.
Standards Exist, Intelligence Doesn't
The HIPAA 276/277 transaction standards were designed to solve exactly this problem. Submit a claim status request, receive a standardized response. No portals, no manual checking, no interpretation needed. The infrastructure works, but the implementation stops at data retrieval instead of extending to decision support.
Current electronic systems essentially automate the wrong part of the process. They fetch status codes faster but still dump raw data onto billing teams who must manually interpret, prioritize, and act. It's like upgrading from a horse-drawn cart to a Ferrari but still making the trip to the grocery store one item at a time.
Primary Healthcare Lens: Provider Operations
The portal proliferation problem exemplifies how healthcare's fragmented payer landscape creates operational complexity that compounds exponentially. Each payer portal has different login requirements, status code formats, and user interfaces. A billing specialist might check Aetna at 9 AM, Blue Cross at 9:30, then UnitedHealthcare at 10, following the same manual pattern across a dozen systems daily.
What's missing isn't better portals. It's intelligent orchestration that converts scattered status data into prioritized work queues where billing specialists focus on judgment calls, not data gathering.
From 24 Minutes to 320 Milliseconds: The Architecture of Parallel Intelligence
The solution doesn't require rebuilding healthcare's payment infrastructure. It requires rethinking how we query and process the data that already exists. Modern API architecture using Promise.all() approaches can retrieve eight claim statuses across different payers in 320 milliseconds while simultaneously analyzing the results for priority and next actions.
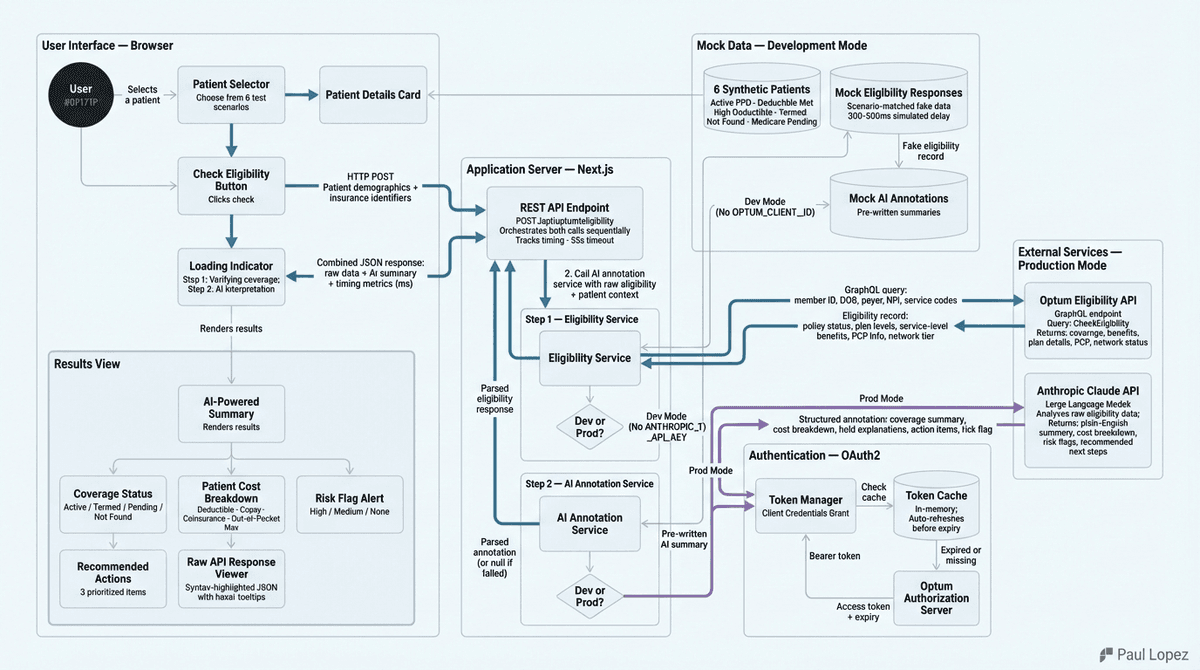
This isn't just speed optimization. It's workflow transformation. Instead of sequential portal checking that consumes entire mornings, parallel processing with AI interpretation creates prioritized work queues. Claude analyzes status codes and generates specific recommendations: "Dorothy Washington - 82 days outstanding, timely filing risk, call immediately" versus "Johnson claim - processing normally, check again in 10 days."
The technical implementation is surprisingly straightforward. The complexity lies in converting status codes into actionable intelligence. A "pending additional information" status might require patient outreach, provider documentation, or payer follow-up depending on the specific context. AI can make these distinctions at scale while humans handle the actual interventions.
Healthcare Implications: Workflow Impact and Economic Reality
This transformation directly addresses healthcare's revenue cycle efficiency crisis. When billing specialists spend 36% of their time on routine status checking, they're not available for higher-value activities like denial appeals, patient payment discussions, or proactive claim correction. The opportunity cost compounds as claims age and collection rates decline.
The economic incentives align across multiple stakeholders. Providers capture more revenue through better claim management and reduced write-offs. Payers benefit from fewer phone calls and portal queries. Patients experience faster claim resolution and clearer financial communication. The constraint has been execution complexity, not regulatory barriers or technical limitations.
Risk management improves significantly when AI monitors all claims continuously rather than relying on periodic human sampling. Timely filing deadlines, missing prior authorizations, and coordination of benefits issues surface automatically rather than during monthly aging report reviews. This shifts billing teams from reactive fire-fighting to proactive revenue optimization.
Measurable outcomes include reduced days in accounts receivable, decreased timely filing losses, and improved billing staff productivity metrics. Early implementations show potential for 40% reduction in status inquiry time while improving claim recovery rates.
The Extractable Skill: ar-claim-prioritizer
The core capability here, ar-claim-prioritizer, is platform-agnostic and integrates with existing revenue cycle management systems without requiring wholesale replacement. It's not about building new infrastructure but about adding intelligence layers to current workflows.
This represents a fundamental shift in how billing specialists spend their day. Instead of opening Portal #1 through Portal #12 in sequence, they receive a prioritized queue with specific action recommendations. The 24 minutes previously spent per inquiry redirect toward activities that actually resolve claims: calling payers, gathering documentation, educating patients, or correcting billing errors.
The beauty of this approach is that it doesn't eliminate billing specialists but elevates their work. Data gathering becomes automated. Pattern recognition becomes systematized. Human judgment focuses on complex cases that require negotiation, relationship management, or clinical context that AI can't provide.
Healthcare organizations implementing similar automation report that billing teams initially worry about job displacement, then quickly realize they're finally able to do the strategic work they were hired for instead of spending all day refreshing browser tabs.
Beyond Status Checking: The Future of Revenue Cycle Intelligence
Dorothy Washington's near-miss represents thousands of similar scenarios playing out daily across healthcare. Claims approaching critical deadlines, patterns indicating systematic issues, opportunities for proactive intervention—all invisible until AI provides continuous monitoring at scale.
The portal infrastructure isn't disappearing, but the manual morning ritual is optional. The question isn't whether this automation is possible (the technology exists today) but whether healthcare organizations will prioritize workflow transformation over system status quo.
Smart healthcare administrators are already evaluating their current status inquiry workflows, calculating the true cost of manual processes, and identifying pilot opportunities for intelligent automation. The ones who move first will capture competitive advantage while others continue logging into Portal #7.
The $12.5 billion question has a clear answer. We just need to stop asking it manually.
References
- CAQH. 2023 CAQH Index Report. 2024.
- MedEvolve. Wasted Touches in the Revenue Cycle. 2024.
- Legal Information Institute, Cornell Law School. 45 CFR 162.1401 & 162.1402
- Equality Health. "Mountains of Paperwork and Multiple Payer Portals." August 2024.
- Physician Leaders. "Clinical Revenue Cycle Analysis." January 2025.